An Introduction to Working with Functional Neurological Disorders
for:
North Staffs Aspiring Psychologist Group


Dr. Chris Gaskell
Senior Clinical Psychologist
Neuropsychology
North Staffordshire Combined Healthcare NHS Trust
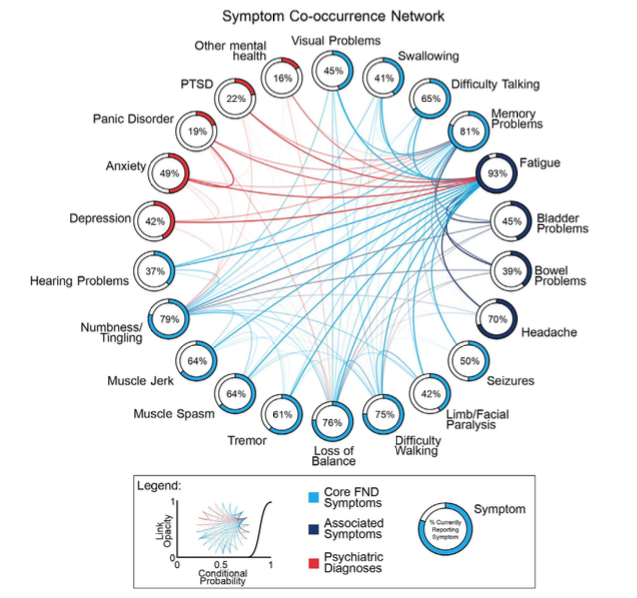
Symptom Heterogeneity
Classified by neurosymptoms.org, extracted 2021
Functional vs. Organic
Functional = Impairment of function.
Not suggesting a behavioural or intentional component.
Functional vs. Organic debates are outdated and inaccurate dualism.1
Can a person be non-organic?2
Software problem vs. hardware problem?

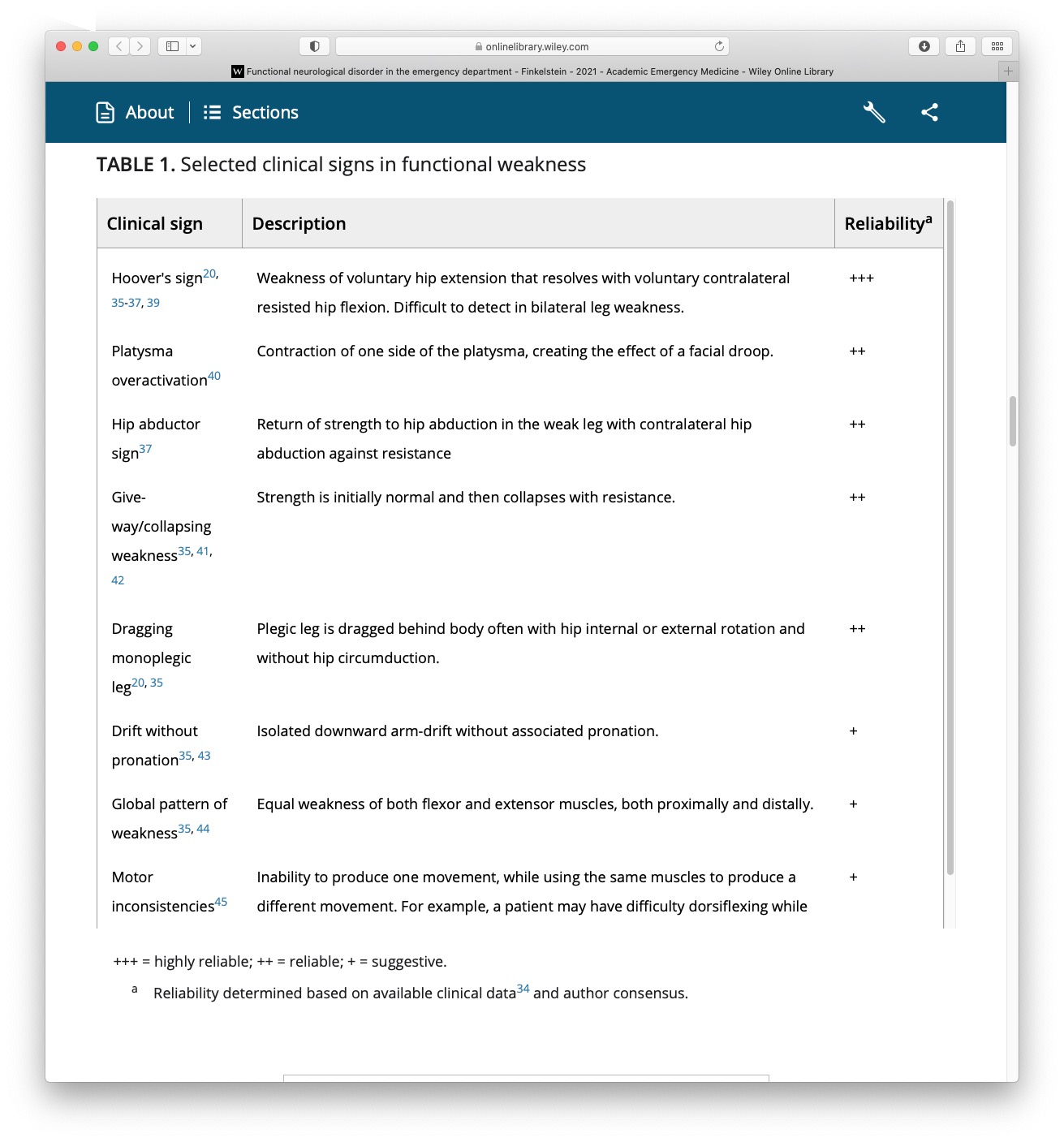
Symptoms: Functional Movement
Taken from: FND in the emergency department Finkelstein et al (2021)
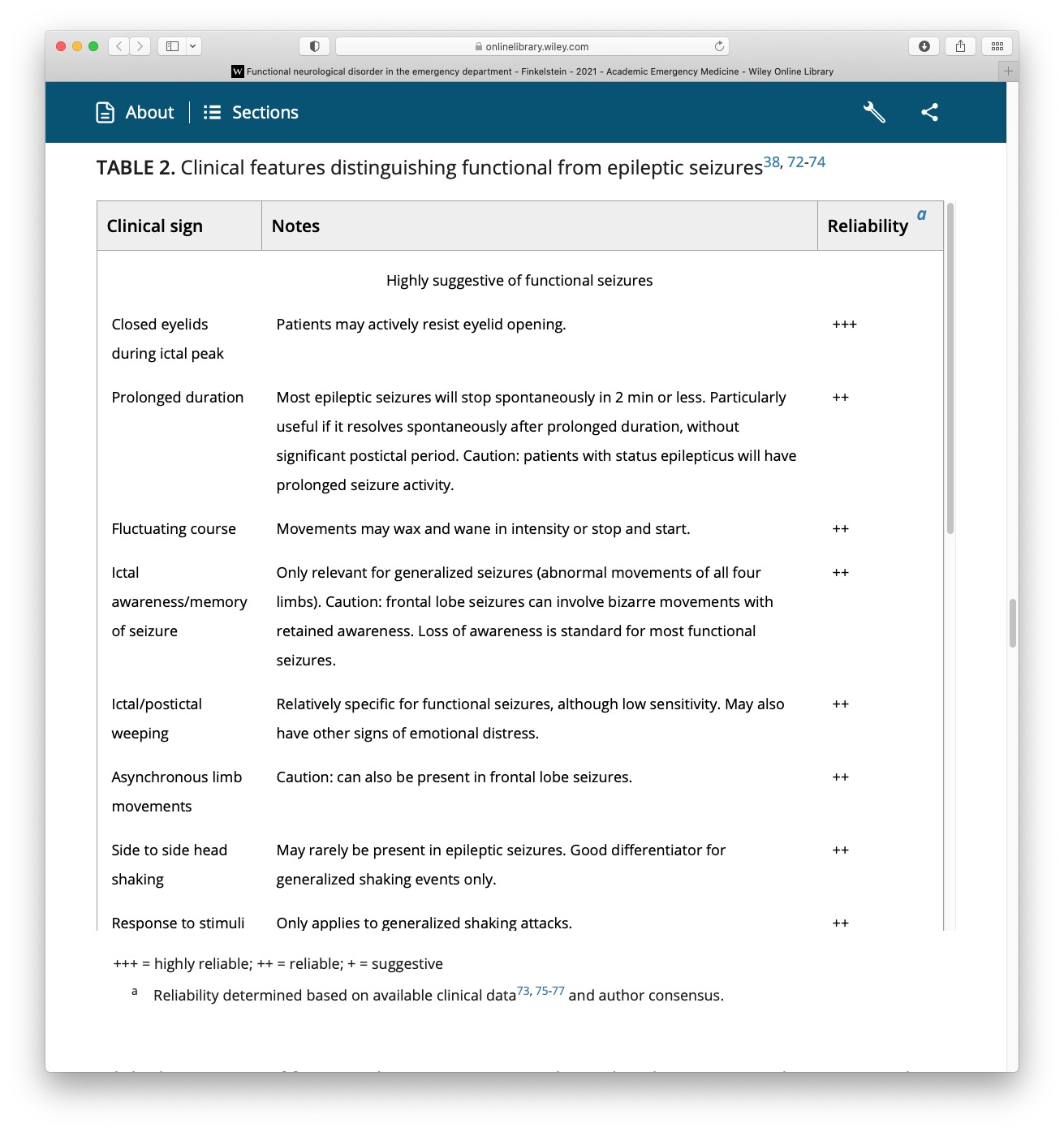
Symptoms: Functional Seizures
Taken from: FND in the emergency department Finkelstein et al (2021)
Terminology and Language
Many terms have been used:
Non-epileptic attacks.
Psychogenic seizures.
Psychogenic non-epileptic seizures (PNES).
Dissociative seizures.
Conversion disorder.
Functional seizures.
Psychological seizures.
Pseudo-seizures.
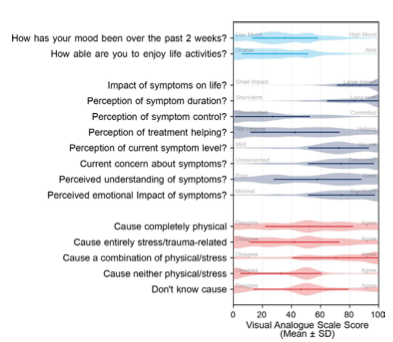
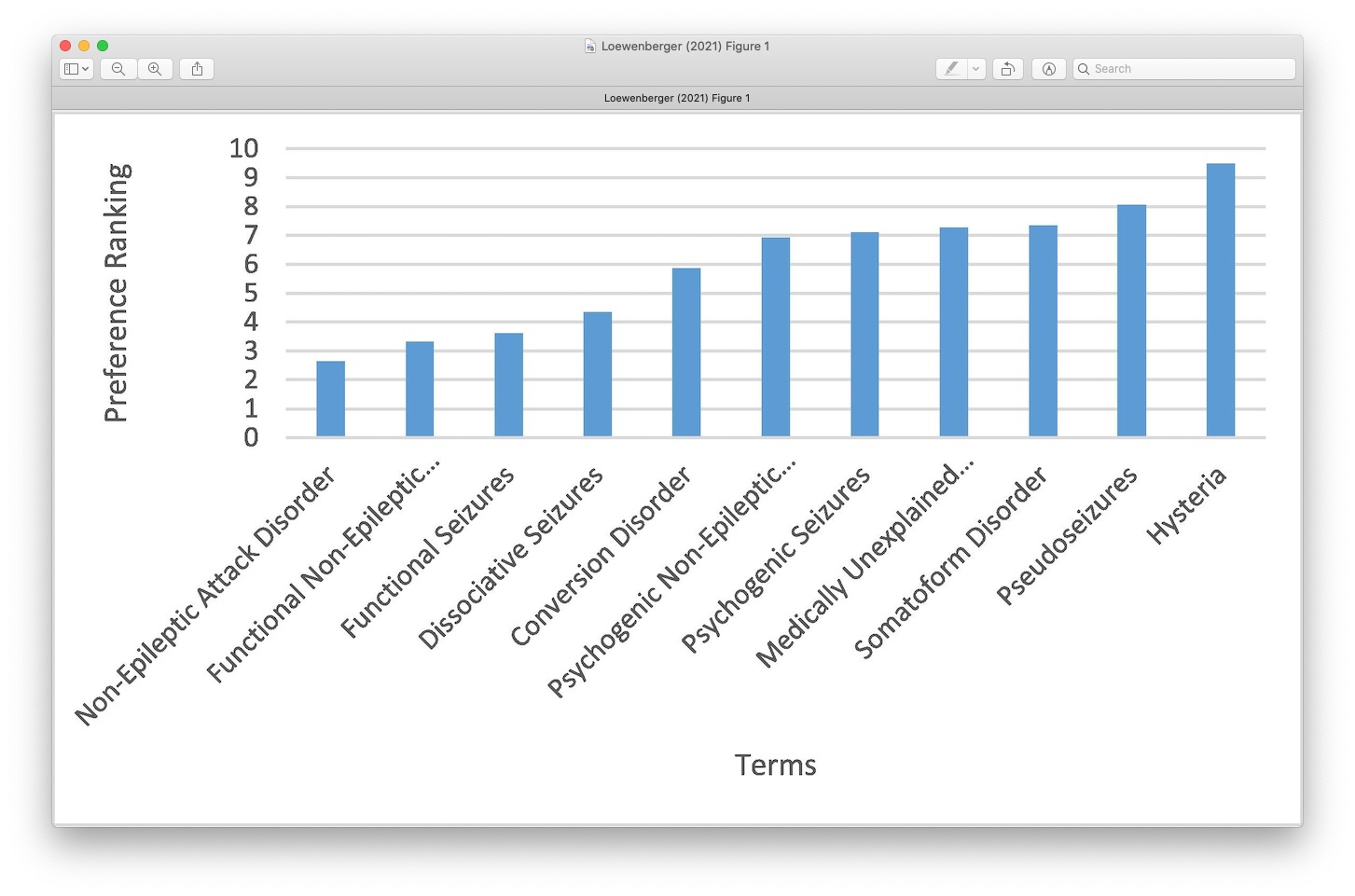
What do Patients Prefer?
Taken from recent Loewenberger, 2021 (UK service evaluation)

The Mind Body Link
Psychological experiences influence the body All The Time.
The cause is not medical but the impact on the body is real.
Sudden shock = heart beats faster.
Embarrassment = face goes red.
Upset = eyes produce tears.
It is normal for changes to happen in the body without a medical cause or disease.
FND also happens through this Mind-Body link.


Autonomic Reactions
Fight/flight/freeze response - evolutionary based fear response that is adaptive for survival.
Freezing is one of the main defensive threat reactions across species
Parasympathetic branch of the nervous system.
A means of responding to a threat or a trigger (at times adaptive)
Rates of Stressful Life Events
Taken from recent Ludwig et al 2018.
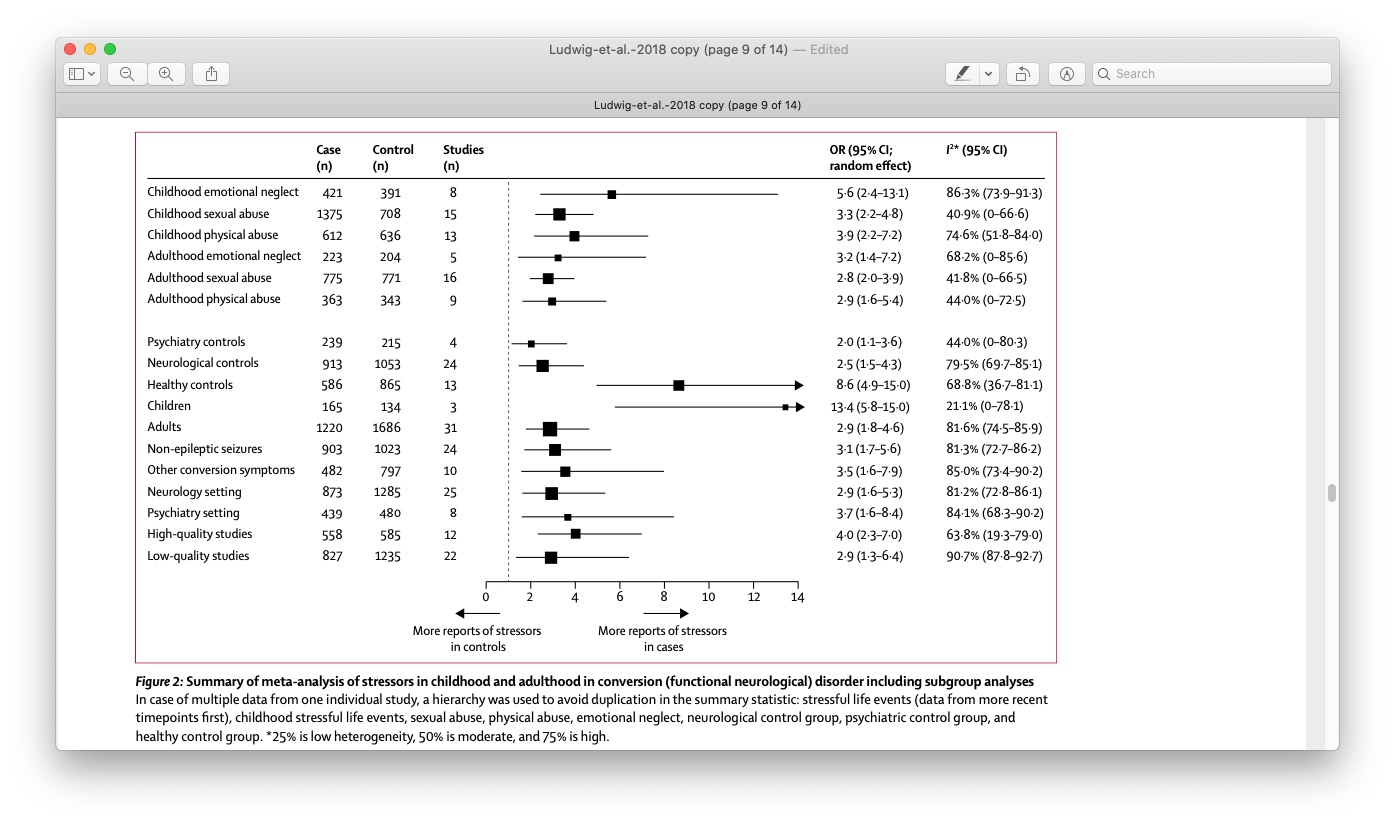
Important Point
Although Rates are high, many people with FND do NOT report having experienced any trauma.
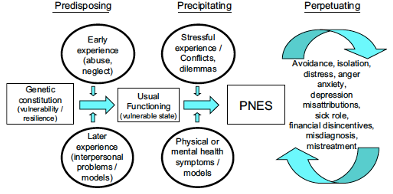
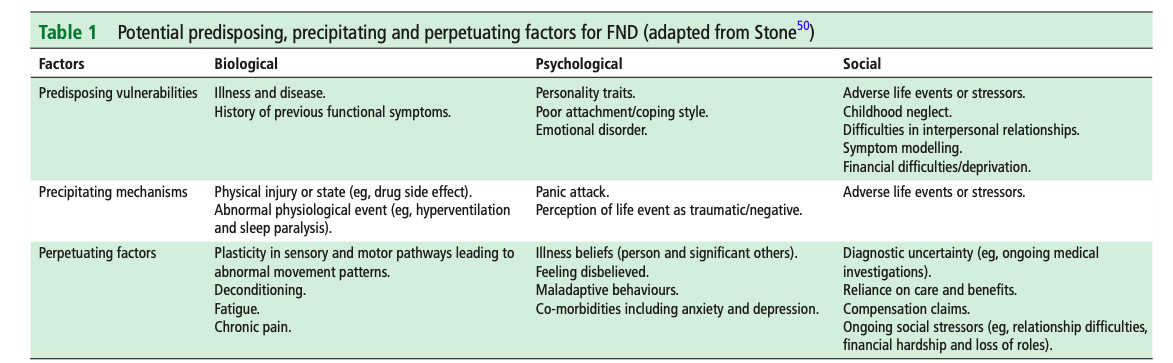
Biopsychosocial & 3 Ps
Taken from Reuber 2009
Taken from Nicholson 2020
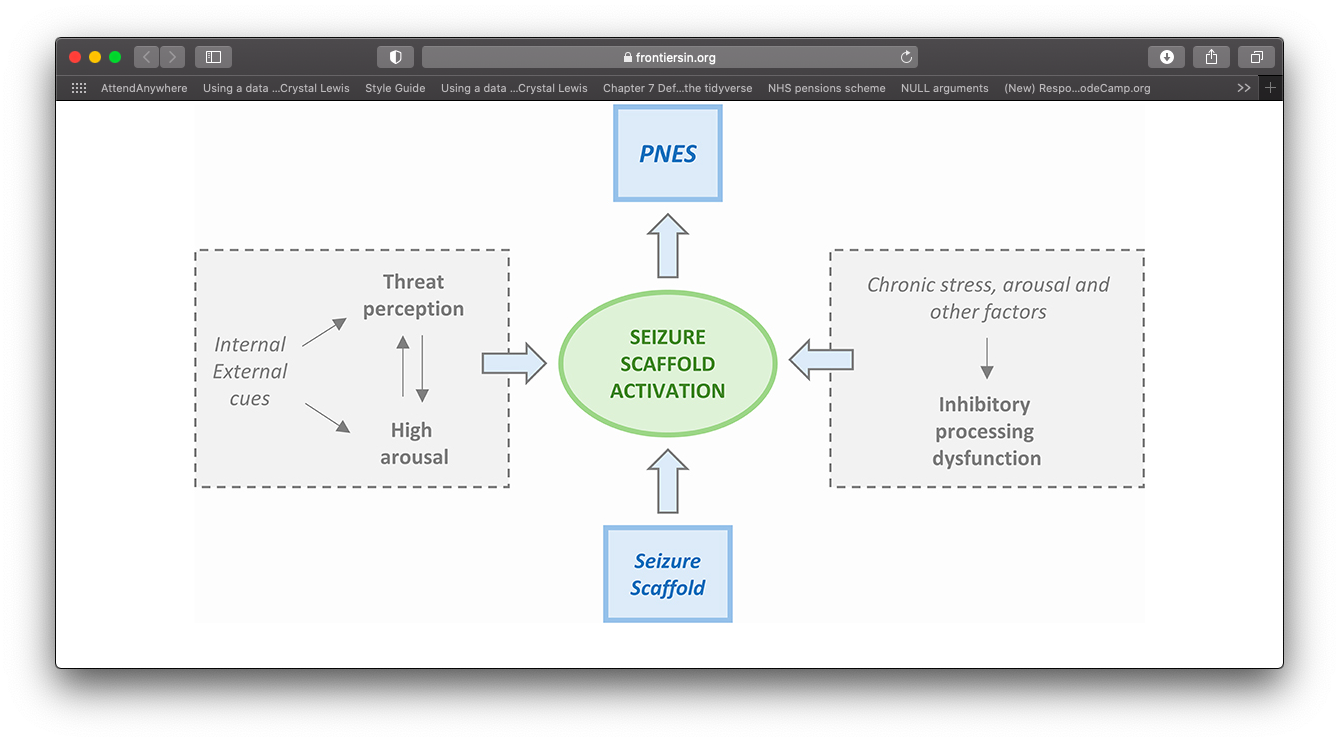
Integrated Cognitive Model
Taken from Anzellotti et al., 2020 (Based on Reuber & Brown)
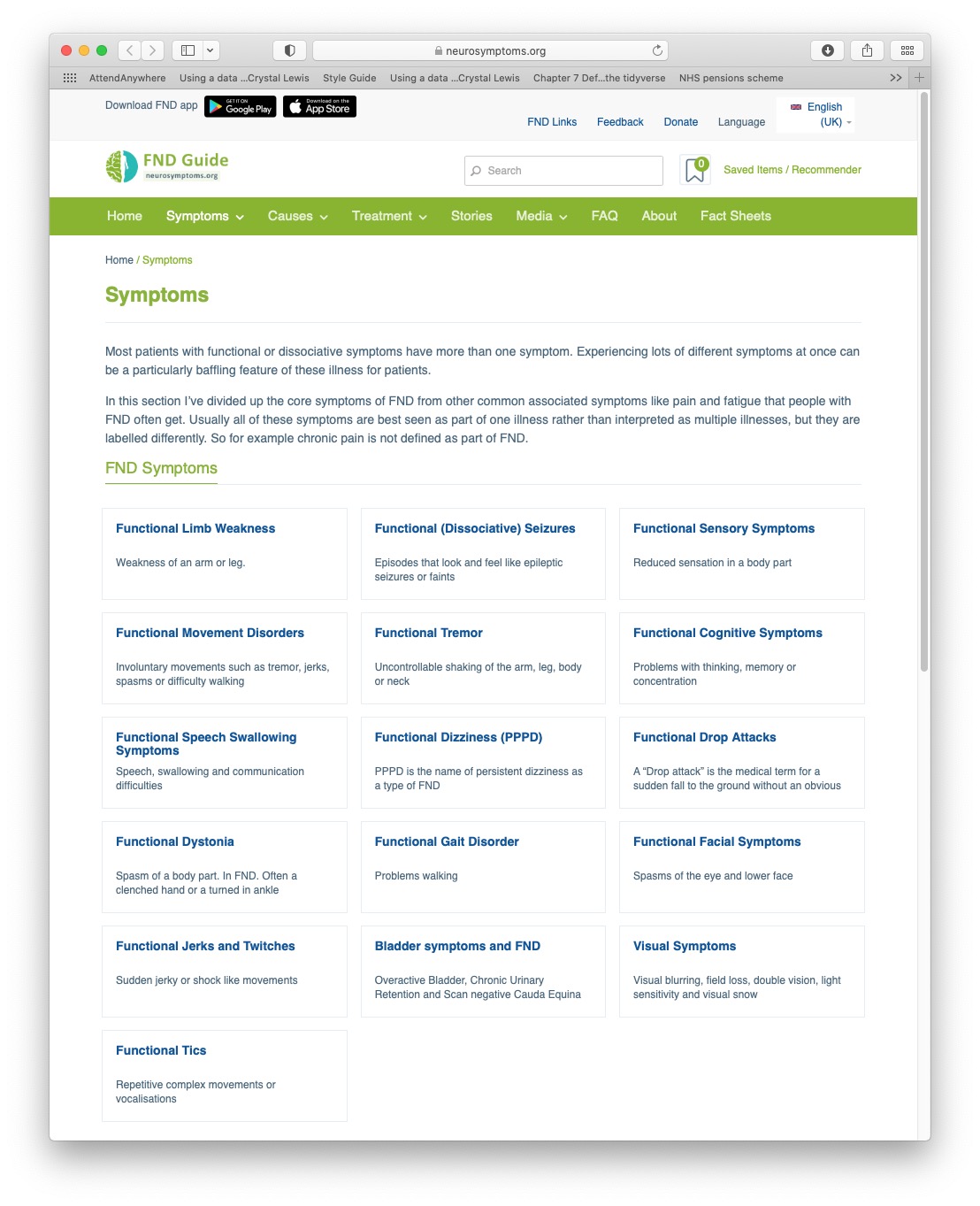
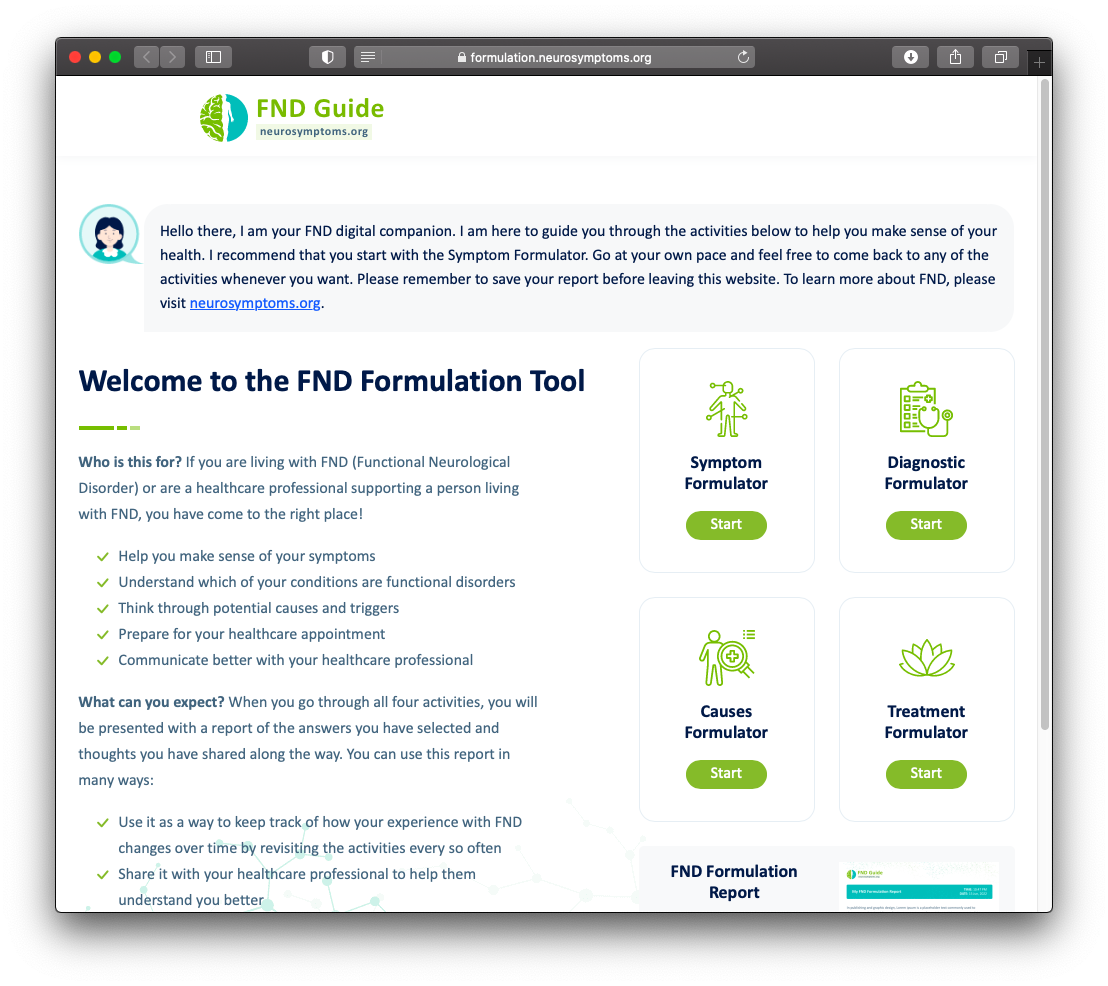
NeuroSymptoms: Treatment Formulator
Support patients to use the newly developed tool from neurosymptoms.org
Role of Psychology
Potentially suited to help all FND variants (won’t be necessary for all).
Co-morbidities needs to be accounted for.
Treating underlying and potentially long-standing distress (e.g., anxiety, depression, trauma).

Websites
FND Hope
FND charity
Lots of helpful information and resources for patients.

FND Society
Professional network for FND
High quality teaching and educational material.

Manchester Neurosciences (Salford NEAD service)
NEAD service website
Information and clinical resources for patients and clinicians.
Neurosymptoms.org
Informational website for patients and professions
Lots of high quality resources and information sheets
